







- Total
- General
- Arts
- Book
- Culture
- Economy
- Essay
- Fun/Joke
- History
- Hobbies
- Info
- Life
- Medical
- Movie
- Music
- Nature
- News
- Notice
- Opinion
- Philosophy
- Photo
- Poem
- Politics
- Science
- Sports
- Travel
Essay Miinnesota Project Professors II--Personal recollections(2)
2018.07.25 12:20
|


Comment 8
-
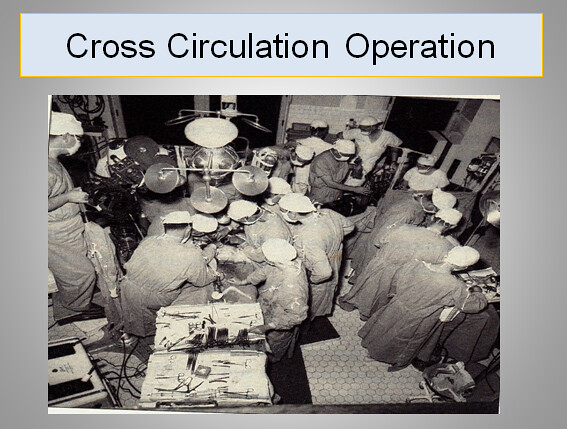
History of Cardiopulmonary Bypass

A heart lung machine used in London's Middlesex Hospital in 1958. Science Museum, London (2008)
An Austrian-German physiologist Maximilian von Frey constructed an early prototype of a heart-lung machine in 1885 at Carl Ludwig’s Physiological Institute of the University of Leipzig.[2] However, such machines were not feasible before the discovery of heparin in 1916 which prevents blood coagulation. A Soviet scientist Sergei Brukhonenko developed a heart-lung machine for total body perfusion in 1926 which was used in experiments with canines. Dr. Clarence Dennis led the team that conducted the first known operation involving open cardiotomy with temporary mechanical takeover of both heart and lung functions on April 5, 1951 at the University of Minnesota Hospital. The patient did not survive due to an unexpected complex congenital heart defect. This followed four years of laboratory experimentation with dogs with a unit called the Iron Heart. A team of scientists at Birmingham University (including Eric Charles, a chemical engineer) were among the pioneers of this technology.[3][4] Another member of the team was Dr. Russell M. Nelson(Current President of The Church of Jesus Christ of Latter-Day Saints), who performed the first open heart surgery in Utah.[5]

Brukhonenko's Autojektor
The first successful mechanical support of left ventricular function was performed in July 3, 1952 by Forest Dewey Dodrill using a machine, the Dodrill-GMR co-developed with General Motors. The machine was later used to support right ventricular function.[6]
The first successful open heart procedure on a human utilizing the heart lung machine was performed by John Gibbon on May 6, 1953 at Thomas Jefferson University Hospital in Philadelphia. He repaired an atrial septal defect in an 18-year-old woman.[7] Gibbon's machine was further developed into a reliable instrument by a surgical team led by John W. Kirklin at the Mayo Clinic in Rochester, Minnesota in the mid-1950s.[8]
The oxygenator was first conceptualized in the 17th century by Robert Hooke and developed into practical extracorporeal oxygenators by French and German experimental physiologists in the 19th century. Bubble oxygenators have no intervening barrier between blood and oxygen, these are called 'direct contact' oxygenators. Membrane oxygenators introduce a gas-permeable membrane between blood and oxygen that decreases the blood trauma of direct-contact oxygenators. Much work since the 1960s focused on overcoming the gas exchange handicap of the membrane barrier, leading to the development of high-performance microporous hollow-fibre oxygenators that eventually replaced direct-contact oxygenators in cardiac theatres.[9](from Internet)
"The first successful mechanical support of left ventricular function was performed in July 3, 1952 by Forest Dewey Dodrill using a machine, the Dodrill-GMR co-developed with General Motors. The machine was later used to support right ventricular function.[6]"
Of note, I was lucky enough to scrub with Dr. Dodrill once in late 1960's during my residency when he was doing an implant of a permanent pacemaker on a patient I was involved in. This was the day the permanent pacemaker implantation required a thoracotomy, and the leads were implanted on the epicardium. The transvenous implantation came later. Dr. Dodrill was in his early 70's and was reported one day in the front page of Detroit News as the first surgeon in the world who invented and used the heart lung machine
along with engineers of General Motors.
-
조동문, 위의 글 잘 읽었습니다. 제가 본과 삼학년 때, 이영균선생님의 첫 mitral valve replacement in Korea 수술을 수술실 윗층 glass dome에서 보았습니다. 미네소타에서 가져온 구형 펌프로 수술하였는데, 장관인 것은 마취교수는(이동식? 조교수) 우리와 같이 2층에 있고, 마취전공의가 bag을 주물럭하다가 어디로인지 가며, 간호사에게 bag을 주물럭하라 하는 걸 보았습니다. 제가 마취과 실습하던 때라 이교수님이 우리에게 지금 무얼 한다고 친절히 말씀하셨지만, 지금 생각하면 정말 한심한 마취였지요. 혈압을 팔에 감은 구형 혈압계였으니요. 전공의는 그 후에 마취과장을 하신 김광우 교수님이고요. 수술 받은 환자는 이영균교수님의 밤새껏 노력에도 불구하고 pulmonary edema로 사망했고, 이영균교수께선 눈물을 펑펑 쏟았다고 신문에 있습니다. 1964년인걸로 기억합니다만.(사실 기억이 가물거려요) 후일 서경필교수님 뵈러 갔다가 이영균교수님도 뵈었습니다.서경필교수님도 스웨덴에가서 현대수술을 배우셨죠.
한중형, 집안의 한분이 이 교수님께 수술을 받았군요. 1970년대엔 수술과 마취가 많이 좋아졌겠지만 몇 백개의 수술이라니 믿어지지 않네요.
하여튼 옛날의 이야기입니다.
신백효
-
Thank you for the comments,Drs,Lee & Shin.
Dr.Lee--It was nice for you to remind other important giants in cardiac surgical history such as J.Kirklin, C.Dennis,R.Nelson,Dodrill---. In contrast to Lillehei, J.Kirklin was a very scientific, methodical surgeon, who built a cardiac empire at Alabama after he left Mayo early 70's----As a long time editor of J.Th.CV surgery since mid 70's, he insisted statistics in all the papers submitted, which was way ahead of other
major clincal journals of internal medical side as well as surgical journals.
Dr Shin--Yes, infrastructure,man-power etc were very poor both in surgical, anesthesia, criticalcare in SNUH those days.
There was no volume controlled respirator, no ABG machine in SNUH proper(one in Pro.고광욱 Lab,),of course no ICU..
On and off,interns and junior residents had to bag all night at the recovery area.
For all the pioneers and professors of those days, probably we cannot & should not make quick judgements on the basis of US standards then, or today's rulers.
Through prof.Lee YK's persistence, in spite of hardships, current level of cardiothoracic surgery in Korea appears remarkable, reaching near top level in global scale, especially in technically challenging procedures such as complex thoracic aortic cases.
Anyway, "Those were the days!"---from "All in the Family "(Arch & Edith Bunker)
-
I was in the same upstairs observation room to see Professor Lee's cardiac surgery.
I am not sure if I was with Dr. B.H. Shin at the same time but probably we were together.
It was because there was a big rumor that there would be an open heart surgery
on that particular time and day. So, many of our classmates were there.
We couldn't see anything from above looking down.
I got out early and later we heard that the patient died.
Then, I felt something strange. My question was that if the surgeon was not sure
on his successful outcome of the surgery, why did he do it?
The SNUH O.R. was not a dog lab !! But it had been being used as a dog lab.
This was what I felt as I was under training in cardiac surgery in the U.S. about 7 years later.
The "fxxxing" authority of an incompetent professor had been good enough
to run a dog lab on human beings !!
As I was interested in getting into cardiac surgery, I was very much interested in those
teaching staffs in the thoracic surgery department.
However, they seemed to be so arrogant and indifferent to the students.
During our student rotation to the department, there were hardly any teachings or personal contacts
between us and them. We were just left alone.
We reported to the Thoracic Surgery ward and there was nothing...
We didn't see the faces of the eminent "dog-lab" professors or anyone of his assistants.
After waiting for a while like orphans in the street, we left school and headed to a billiard parlor.
The stories were very similar in all other clinical departments.
However, we were paying dear money we earned by tutoring in our spare time.
Later, as I became a thoracic surgeon, I realized that probably none of them knew enough to teach us.
It's a sad story in those days of around 1964.
These guys were hanging in there with all those fake authorities and undeserving seniority.
From across the Pacific, as I was being taught and learning civilized U.S. medicine,
I was realizing how ignorant the teaching staffs of SNU MC were during those days.
The medical school let everyone to pass the semester examinations by keep repeating re-exams.
There were, eventually, no students who flunked the class.
Later, I came to a realization of their policy of "no flunking".
It was meant to cover up their incompetence. I am pretty sure about that.
Only guys who flunked were those who were not able to pay the darn tuitions.
Here, I am talking about those days before and around 1964.
What happened after 1965, I do not know but it should have improved.
I assume it might have been getting better when there was a policy of getting rid (forced retiring)
of those professors at age 65 and over, the trashy and withered remnants of Japanese era.
Those experiences and negative feelings during the medical school days kept me from the yearning
for the nostalgia. Thus, unfortunately, I do not have many fond memories of my medical education in Korea.
Anyway, whom can I blame now? It was just bad old days for us.
I am glad that I got out of it quickly and got into the civilized American medicine.
I hope the uncivilized and ignorant time are forever over and no more in Korea nowadays.
-
"if the surgeon was not sure on his successful outcome of the surgery, why did he do it?"
There is no easy answer to this question. Big medical ethics question?
This happened in USA also back then and happens even now, maybe lesser degree, in different
area in different forms ,especially in surgical area, all those sexy new operations----
.
Charles Baily, who did the first series of closed mitral commisurotomy in late 40’s and ealy 50’s,
lost many patients, especially 4 deaths(Hahneman) before the first successful case at the
Episcopal Hospital in Philadelphia. Probably he could not continue the experiment(?) at
Hahnemann,
He was a controversial figure due to the uncompromising, volatile, aggressive relationship, loosing
hospital privileges at some of the Philadelphia area hospitals in late 40’s and early 50’s. Moved to
New York and later he became lawyer in 70’s, maybe due to the turbulent experiences.
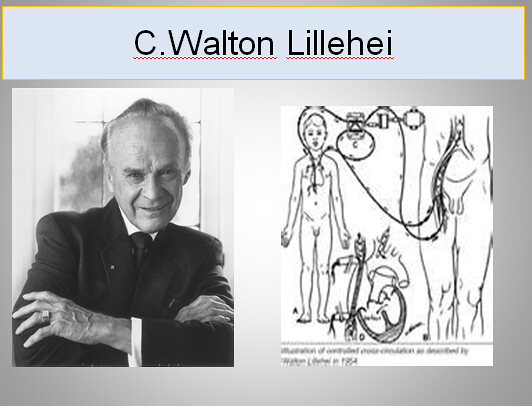
Lillehei was not sure if he would be successful in the first attempt of the cross circulation case
,asked permission of chairman, Dr. Wangensteen to do the first case. The famous memo from the
Legendary Chief on a piece of paper “Dear Walt. By all means,go ahead, O. W”. apparently still
exists.
Mortality was still high 30-40%.
Some nurses at U of Minn. called Lillehei “murderer”. One mother became vegetable from air
embolism CVA. When Lillehei presented C.C cases in American College of Surgeons, some
surgeons shouted & questioned ethics of Mother death(mortality 200%-issues”
Recently, I saw a 3-4 year old boy during Mongolian trip, a case of huge pelvic-retroperitoneal
sarcoma , neglected, untreated, invading sacrum, protruding through perineum, obvious case of
sarcoma.
No money. Young parents. The father , a shepherd tending sheeps and horses on the remote
Mongolian prarie. If I were a surgeon there, I might take the boy to surgery even though I did
not have too much experience on similar cases with chances of long term survival unlikely., high
operative mortality. Adjuvanct chemotheraphy, adjuvanct RT—all luxuries in the book
unavailable or not affordable--
So called National Mongolian Health insurance runs about after 3-4 doctor visits a year.
Rest of expense from out of patients’ pocket.------- Reminded me of old Korea we grew up.
Interesting story I heard from a general thoracic surgeon of Univ. of Chicago Medical school.
In 1970's, graduating class students of the prestigious medical school put a performance/show to the professors
depicting each department.
When cardiac surgery depatment session came, students put a performance,send a patient into OR---
comes out on a stretcher covered with white sheet--to morgue...,,another patient --comes out same way----
next patient comes out same way on a stretcher covered with white sheet---to morgue-----ㅎㅎㅎ
I'd like to see the faces of those famous professors at that moment.
Again,"those were the days'--"All in the Family!"
-
We have lived through many strange periods in Korea as well as in America.
Many times, those were sad and tough times.
But thinking about what we are today, those past events of ours might have been blessings in disguise.
Or we could say that we had overcome all those by learning, working hard,
and eventually defeating our adversaries.
Through the hells and to be what we are today, I believe myself and my classmates have been very lucky.
We are just carrying some bad memories and bitter smiles.
The main thing is that we stay happy and proud.
-
조중행 박사와 같은 시대에 서울대학병원에서 수련의 과정을 겪고
수많은 밤을 잠도 못자며 일하던 시절이 생각 납니다.
그 당시 마취 수련의 로서 심장 수술 마취를 하면서
길면 12-14 시간씩 걸리며 하는 수술후에 환자가 회복실에서 사망하면
통탄해 하시던 이영균 교수님의 모습이 생각 납니다.
이 교수님은 그 더러운 시궁창물 같은 대(?) 서울대학병원에서
제가 존경 하던 몇 않되던 교수이자 학자이시던 분이었습니다.
나중에 제가 서울 대학병원에서 조교수로 근무하며 본 서울대학병원은
우리가 학생/수련의 로서 바라보던 것 이상으로 썪고 더러운
시궁창물 같은 곳이었습니다.
그래도 이영균 교수님은 역시 제가 존경해야 할 분이셨습니다.
조중행 박사가 그런 훌륭한 분 밑에서 심장외과의 로서 기본 수련을 받은 것이
조박사가 미국에 와서 심장외과 전문의로서 성공할수 있었던
밑걸음이 되었던 것이 아닌가 하고 생각 해 봅니다.






| No. | Subject | Date | Author | Last Update | Views |
|---|---|---|---|---|---|
| Notice | How to write your comments onto a webpage [2] | 2016.07.06 | 운영자 | 2016.11.20 | 18164 |
| Notice | How to Upload Pictures in webpages | 2016.07.06 | 운영자 | 2018.10.19 | 32306 |
| Notice | How to use Rich Text Editor [3] | 2016.06.28 | 운영자 | 2018.10.19 | 5890 |
| Notice | How to Write a Webpage | 2016.06.28 | 운영자 | 2020.12.23 | 43809 |
| 365 | I Lift My Lamp Beside the Golden Door [10] | 2018.12.16 | 정관호*63 | 2023.08.01 | 643 |
| 364 |
Crossing George Washington Bridge via Pedestrian Walkway
[3] | 2018.12.12 | 정관호*63 | 2023.08.01 | 831 |
| 363 |
Walking across the Brooklyn Bridge
[5] | 2018.12.11 | 정관호*63 | 2023.08.04 | 478 |
| 362 | 고향의 벗 | 2018.12.07 | 노영일*68 | 2018.12.08 | 112 |
| 361 |
I crossed the George Washington Bridge
[4] | 2018.12.06 | 정관호*63 | 2023.08.28 | 6267 |
| 360 |
[잡담] My Failed Crossing of George Washington Bridge
[4] | 2018.12.03 | 정관호*63 | 2023.08.01 | 10452 |
| 359 | 늦가을 1, 2014 [5] | 2018.11.21 | 조중행*69 | 2018.11.24 | 189 |
| 358 | 늦가을 (2),2018 [5] | 2018.11.18 | 조중행*69 | 2018.11.19 | 139 |
| 357 | The Story of Saber Fighters [16] | 2018.11.13 | 정관호*63 | 2024.02.24 | 608 |
| 356 | 졸업 50 주년 기념행사 후기 [6] | 2018.10.26 | 노영일*68 | 2018.11.13 | 156 |
| 355 | 고향 하루 방문기 [5] | 2018.10.26 | 최광택*70 | 2019.07.05 | 453 |
| 354 | 우리들의 노년을 맞이하고 보내면서 [9] | 2018.10.14 | 이광선*65 | 2018.11.05 | 286 |
| 353 | September 2018 & my Walk [5] | 2018.09.17 | 조중행*69 | 2018.09.18 | 246 |
| 352 |
[잡담]왕소군의 슬픔: 그때 서양은?
[6] | 2018.09.16 | 정관호*63 | 2023.08.02 | 162 |
| 351 | 서재필 & 파친코 [4] | 2018.09.13 | 조중행*69 | 2018.09.14 | 169 |
| 350 | 꽃밭 [6] | 2018.09.05 | 노영일*68 | 2018.09.13 | 114 |
| 349 |
[잡담] 조강지처
[6] | 2018.09.04 | 정관호*63 | 2023.08.29 | 130 |
| 348 | 여름 2018 [7] | 2018.08.18 | 노영일*68 | 2018.09.01 | 156 |
| 347 | 한 진보 정치인의 자살 과 정치인의 눈물 [5] | 2018.08.16 | 조중행*69 | 2018.08.16 | 141 |
| » | Miinnesota Project Professors II--Personal recollections(2) [8] | 2018.07.25 | 조중행*69 | 2018.08.12 | 260 |
Thank you, Dr. Choh, for your enlightening us once again with memorable stories
concerning the beginnings of the cardiac surgery in Korea by Professor Lee.
Personally however, it brings back to me a sad memory involving my older sister
who died 3 days after mitral valve replacement for severe mitral stenosis by Professor Lee in mid 1970's.
As a brother who is a cardiologist, this was one of my greatest regrets in my life.
My sister had been under the care of 최규완교수님 for years for mitral stenosis,
and I was in the process of having her come to Detroit where I was practicing.
I still remember the words by Prof. Choi saying that Prof. Lee had done over 500 cases
of MVR with a mortality comparable to American surgeons less than 10% or so.
My sister developed an unexpected difficult to control uterine bleeding from high venous pressure
preventing her from coming to America, which led to the surgery by Prof. Lee.
As you illustrated well, I gather so many patients including my own sister had to pay
with their lives for the advancement of the early cardiac surgery in Korea.