







- Total
- General
- Arts
- Book
- Culture
- Economy
- Essay
- Fun/Joke
- History
- Hobbies
- Info
- Life
- Medical
- Movie
- Music
- Nature
- News
- Notice
- Opinion
- Philosophy
- Photo
- Poem
- Politics
- Science
- Sports
- Travel
Medical [Medical] Cataract Surgery Informations
2016.11.01 00:55
Considering cataract surgery? What you should know
The operation to replace a clouded lens is low-risk, fast, and effective, but requires some decision making.

Image: CJ_Romas/ Thinkstock
Cataract surgery—which involves removing the eye's clouded lens and replacing it with a clear synthetic version—once required several days in the hospital and a long recovery period. Today it is performed under local anesthesia on an outpatient basis, and people are back to their normal lives within days. The success rate is high, and the rate of vision-threatening complications is relatively low. For people with cataracts, the decision whether to have surgery may be easy to make. However, two additional decisions might be more difficult: when to have surgery and what type of lens implant to get, says Dr. Laura Fine, an ophthalmologist at Harvard-affiliated Massachusetts General Hospital.
Why you may need cataract surgery
To a great extent, cataracts are a normal consequence of aging. Cataract formation is usually a gradual process that plays out over years. The lenses of our eyes become less transparent, less resilient, and often thicker. By age 80, half of us will have cataracts.
Cataracts can creep up on you. It may be hard to tease out the effects of a developing cataract from other age-related vision changes. In the early stages you may become more nearsighted, a problem that can be corrected with glasses. As the cataract progresses, your night vision may worsen, and colors may appear duller.
Any vision changes warrant an eye exam. However, because cataract-associated changes can be subtle, it's better not to wait until your sight is noticeably affected. Comprehensive eye exams, which can detect not just cataracts but also glaucoma and other eye conditions, are recommended every two years for adults ages 40 through 64 and annually for everyone 65 or older.
The doctor will test the sharpness of your vision by having you identify a series of symbols or letters on a chart. He or she may also dilate your pupils with drops to examine the interior of the eye. Using a slit lamp—to illuminate a small area inside the eye at a time—the doctor can see any cataract and assess how extensive the clouded areas are. Additional examinations and tests help rule out other eye disorders, such as glaucoma or retinal degeneration.
 When do you need a lens replacement?
When do you need a lens replacement?
Removing and replacing the clouded lens is the only effective cure for a cataract. For most people, the question is when to undergo the procedure. "There's no rush to have cataract surgery. It isn't a life-threatening situation," Dr. Fine says. That decision is usually based on how much the cataract is interfering with your vision and daily life. You may want to delay cataract surgery until you feel that you need better vision. But you might not want to wait until you can't see stair steps clearly or fail a driving test. If you have another eye condition, such as age-related macular degeneration, your doctor may recommend cataract surgery sooner because the cataracts make it difficult to examine and manage the other problem.
If your doctor determines that you have cataracts in both eyes, he or she may recommend operating first on the eye with the denser cataract. If surgery is successful and your vision improves substantially, you may elect to forgo surgery on your other eye. However, most people get significant benefits from having the second eye operation, including better depth perception and improvements in their ability to drive and to read. People usually have the second surgery once the first eye has healed and their vision is stable. If you are extremely far-sighted or nearsighted and need cataract surgery in both eyes, you may want to have the second surgery within a month or so of the first surgery to avoid problems with double vision and depth perception due to the difference in vision from eye to eye.
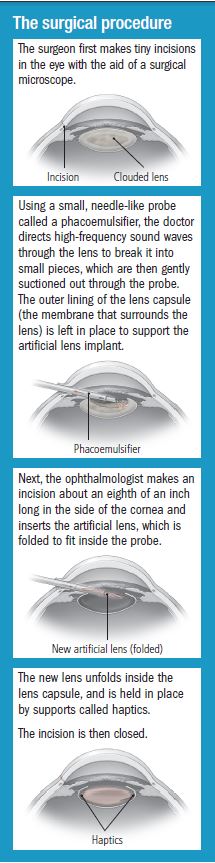
What's involved in cataract surgery
Experience and technology have fine-tuned the procedure to replace the eye's lens so that it takes only about 15 minutes to perform. The approach used most often is phacoemulsification—informally known as phaco. It offers good long-term results, and 97% to 98% of all cases done by an experienced surgeon are successful and free of complications.
The recovery period
You'll spend about an hour in the recovery room as the anesthesia wears off. The doctor may place a bandage or clear shield over your eye. You'll need to have someone help you get home.
Once at home, your primary goal will be to keep your eye from getting infected. You'll need to use eye drops several times a day and to keep water out of your eye. You can go about your daily routine as long as you avoid heavy lifting or activities like jogging that can jar the new lens.
It's also fine to read and watch TV by the day after surgery. The first thing you're likely to notice is how vivid colors seem and how much more detail you can see.
Your surgeon will probably ask you to return for a check-up the day after surgery, a week later, and a few weeks after that.
Making the lens choice
"The primary goal is to improve your vision and function," Dr. Fine says. There are several things to consider when you're choosing a lens, especially these points:
What's most important to you. For most people, the monofocal implant is a good choice, Dr. Fine says. It provides the best contrast vision, so it's good for driving and most other activities. It's also a good choice for people who have cataract surgery when they are relatively young, because contrast vision is likely to diminish with age. However, many people who have monofocal lens implants still need glasses for reading or distance. Multifocal lenses may be a good choice if you do lots of close work, don't want to use glasses, and accept less visual clarity as a trade-off.
Cost. Insurance typically covers monofocal lenses, but you can expect to pay about $1,500 for each toric lens and about $3,000 apiece for other specialized lenses.
The surgeon's experience. Because specialty lenses are newer and relatively few people choose them, many surgeons have limited experience placing them. If you're considering one, find out how many such implants your surgeon has performed.
Commonly used replacement lensesAs the number of cataract surgeries has grown, so have the options for lenses. The most widely used include the following: Fixed-focus monofocal lenses. These lenses can help you see at a distance, but you'll need reading glasses to see up close. Alternatively, some people who get fixed-focus monofocal lenses have one eye fitted with a lens that provides near vision and the other eye with a lens that provides far vision. This com-bination is called monovision. If you are considering this option, your eye surgeon may recommend that you try out monovision with contact lenses before your cataract surgery to see how well you can adjust to the combination. Monovision is usually not an ideal option for people who require crisp, detailed vision. Accommodating monofocal lenses A newer option, accommodating monofocal lenses, can shift from near to far vision in response to movements of the ciliary muscles in your eye, similar to the natural lens in a younger eye. These lenses offer excellent distance and middle vision, but they aren't as reliable for near vision. Eye exercises can help you get used to them, but about half of people who receive them still end up needing reading glasses. Toric lenses These specialized monofocal lenses are designed for people with astigmatism. Toric lenses offer focused vision at a single distance and correct your astigmatism, so you might not need distance glasses after surgery. Multifocal lenses Like the bifocal or progressive lenses used in glasses, multifocal lenses have different areas designed for distance, intermediate, and near vision. The brain and eye figure out which part of the lens to use. The main drawback of multifocal lenses is they can distort bright light, creating more glare and halos at night. |
Originally published: October 2016
Comment 6
-
이한중*65
2016.11.01 01:01
-
이한중*65
2016.11.01 07:06
-
황규정*65
2016.11.01 21:37
This information is very useful and a guideline for helping me to decide in the future.
Also
We all appreciated your continous efforts for the pertinent health informations to senior like most of us.
Keep up the good work! Thanks. KJ
-
이한중*65
2016.11.01 23:39
Daily Statin Might Raise Your Risk for Cataracts
But benefits of cholesterol-lowering drugs outweigh risks, experts say
WebMD News Archive
WebMD News from HealthDayBy Steven Reinberg
HealthDay Reporter
FRIDAY, Dec. 5, 2014 (HealthDay News) -- Taking a statin to lower your cholesterol may raise your risk of developing cataracts, Canadian researchers report.
While statins such as Zocor, Crestor and Lipitor protect many people from heart attack and stroke, they may raise the odds of developing the vision problem by 27 percent, the researchers report.
But the risk of developing cataracts -- a clouding of the lens of the eye -- is insignificant compared with the benefits of these drugs, said lead researcher Dr. G.B. John Mancini.
"The benefits of statins are far outweighed by any small risk for cataract surgery," said Mancini, a professor of medicine at the University of British Columbia in Vancouver.
"However, the indication for statin use should be solid from the outset and fully understood by patients," he added.
Mancini said this study can't prove that statins cause cataracts. "Careful observations in clinical trials are needed to support or refute this association," he said.
Dr. Mark Fromer, an ophthalmologist at Lenox Hill Hospital in New York City, said cataracts are very common. "In one's lifetime, the chance of developing a cataract is 100 percent," he said.
"The goal is we want to keep you alive long enough to get one, and that's where statins come in," he said. "Statins increase the length of life by decreasing strokes and heart attacks."
Cataracts can be treated with surgery that is "quick, painless and 99.9 percent successful," Fromer said. "So, since you are going to get a cataract anyway, you might as well take your statin -- it's in your best interest."
The study was published in the December issue of the Canadian Journal of Cardiology.
For the study, Mancini's team used the British Columbia Ministry of Health database from 2000 to 2007 and the IMS LifeLink U.S. database from 2001 to 2011. In all, they looked at more than 207,000 adults with cataracts and more than 1.1 million without them.
Among people in the Canadian database, those who took statins for at least a year had about a 27 percent increased risk of developing cataracts that needed surgery, compared with people not taking statins. The increased risk for patients in the U.S. database was only 7 percent, but that was still statistically significant, the researchers said.
-
이한중*65
2016.11.01 23:48
Dr. Hwang,
I appreciate your comment.
We are all getting old together.
I would like to continue to remain as a medical student learning everything related to medicine,
looking at our aging bodies and minds as research subjects and for my personal observation
as a medical student as an extension of my dream when I entered the medical school.
-
이한중*65
2016.11.02 00:15
Fit Exercise into Your Life for Healthy Body, Healthy Eyes Most of us know that eating right and exercising lowers our risk of illnesses such as heart disease, diabetes and numerous other health problems associated with obesity. What should come as no surprise is the importance of living a healthy lifestyle and how it is directly related to maintaining all of your body’s organs, including your eyes.
Even though research is still in its preliminary stages, evidence shows that those with an active lifestyle have better eye health and are less likely to develop an eye disease later in life than those that lead a sedentary lifestyle. The reason for this is a simple one. Increasing your heart rate through vigorous aerobic exercise causes more blood to be adequately pumped through all parts of the body, including the eyes. This process actually stimulates the eyes promoting better eye health and improving your vision.
Numerous studies have indicated that aerobic exercise benefits eye health by:
⇝Reducing the onset of cataract formation
⇝Providing a new approach in the prevention of age-related macular degeneration
⇝Effectively and easily reducing the eye pressure in glaucoma patients
⇝Preventing diabetes by maintaining a healthy weight and keeping blood sugar levels under control
Guidelines suggest aiming for a minimum of 30 minutes of aerobic exercise or performing a low-intensity form of exercise such as walking for at least 45 minutes five days a week, if not daily.
Are you already physically active? Great! Then you are reaping all of the fabulous benefits exercise provides. If not, fitting exercise into your daily routine to improve your overall health and well-being is as simple as finding activities that you enjoy doing.
For motivating ways to stay active and ideas on how to stay committed to your exercise program and your weight loss journey, visit SparkPeople.com. This website not only offers an abundance of nutrition and exercise resources, but also includes motivational blogs and even chat rooms. This free online diet and healthy living community is a network of personal trainers, medical experts as well as nutritionists available to you at any time to help you live a healthier life and reach your goals.
The bottom line is exercise strengthens not only your body, but also your eyes. So once again, exercise is the defender in taking the title for benefiting your overall health and well being.(from Internet)............
I have early cataracts for at least two years eye doctors are more than happy to do cataract surgeries on
that I am observing.
I have taken statins for at least twenty years and at the same time
have maintained regular aerobic exercise program.
My personal observation in regard to the benefit of exercise
slowing down the progression of cataract is positive
although perhaps limited against aging.
One observation I make frequently, for example, is that the blurred vision I get from reading would clear up
once I exercise to the point of sweating.
I believe this article provides useful informations to those of us,
including me, considering cataract surgery.